While CAR T cell therapy has revolutionized treatment for many blood cancers, including (NHL), many patients who receive CAR T cell therapy do not experience a long-term remission. For those whose cancers return or become resistant after CAR T cell therapy, the prognosis is poor, with few options left.
A new “armored” form of CAR T cell therapy, developed by , the Richard W. Vague Professor in Immunotherapy in the Perelman School of Medicine at the University of Pennsylvania, may be able to help these patients. According to the results of a , presented today at the ( ), the new CAR T was safe, and had a three-month overall response rate of 80 percent in 20 patients with NHL whose cancers were relapsed or had stopped responding to treatment after receiving a commercially available CAR T cell therapy.
“By the time we treat someone with commercially available FDA-approved CAR T cell therapies, they’ve already tried at least one other treatment that either didn’t work at all or their lymphoma relapsed, and they’re very hopeful that CAR T cell therapy—which has made such a difference for so many—will work for them too,” said , an associate professor of Hematology-Oncology, who led the clinical trial at Penn Medicine’s . “If the standard of care CAR T cell therapy doesn’t work for them, it’s incredibly disappointing. While we still have more follow-up to do, it’s gratifying to see so many patients with lymphoma responding to this novel CAR T cell product developed here at Penn.”
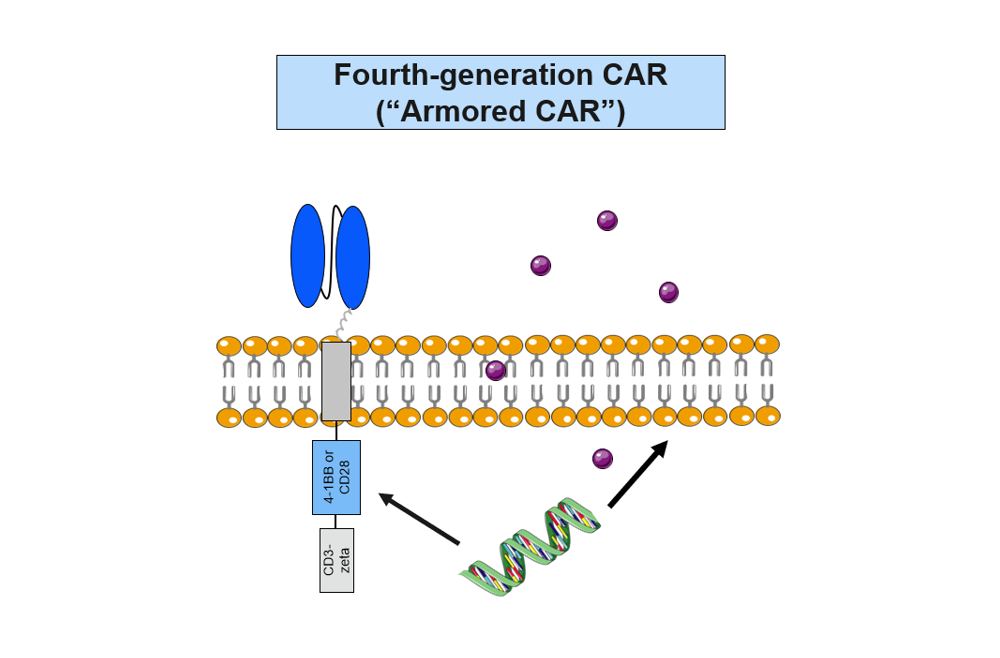
The first-in-human study evaluated huCART19-IL18, an anti-CD19 CAR that was further modified to secrete the pro-inflammatory cytokine, interleukin 18 (IL 18), based on preclinical studies that showed it could enhance CAR T activity.
“We’ve likened this CAR T to an armored truck or tank because the release of IL 18 further protects the CAR T cells and promotes their ability to attack the cancer cells,” said June, whose pioneering research led to the .
The production of huCART19-IL18 also uses a process, developed by Penn’s , that shortens the manufacturing time for the CAR T cells to three days. For patients with aggressive, fast-growing cancers, this means being able to begin CAR T cell therapy quicker than is currently possible with standard manufacturing times of nine to 14 days. A found the shortened manufacturing time also may enhance the potency of the T cells.
The addition of IL 18 did not result in any new or unexpected safety concerns beyond the known side effects of CAR T cell therapy, including cytokine release syndrome (CRS) and neurotoxicity, which were managed successfully. As patient follow-up continues, the median overall survival after treatment has not been determined yet, with some of the earliest patients treated now in remission for two years or more.